2 Years on ……
I have now been qualified and operating as a SyncEquine Thermal Imaging Technician for 2 years. Cliche I know, but how time flies and there has not been a day I have regretted the decision to join the SyncThermology team.
Over the last 2 years I have met and worked with some lovely clients, professionals and indeed horses who I always find so endearing once they relax and take on their role of super model.
Sync’s team of vets offer excellent support and are always available to discuss and offer advice on each case. As well as educating the team by giving presentations and live dissections at company CPD’s and team webinars. I find each case fascinating and as my veterinary knowledge increases so does my passion for learning more. If you are like-minded and would like to see how our screening service can benefit the equine veterinary industry. Please read on!
In this blog I would like to share with you a handful of cases I have had the pleasure of being involved with. Each being a reflection of some common veterinary issues I regularly come across along with some unexpected diagnosis’. Soon after starting this blog I also realised are naturally linked to the company’s quarterly themes, in particular: Joint Disease, Pain or Behaviour, Poor Performance, Tendons & Ligaments and Detecting Early Pathology
Below are a summary of four cases, where I have pulled out the most relevant points from the SyncEquine Veterinary reports to share with you.
Case 1 August 2016 – Joint Disease/Poor Performance
My first client and scan I performed as soon as I had finished my training . Myself and my client were both surprised to say the least at the findings. We were both convinced there was something going on in this mare’s back, which we were not completely wrong, But strongly reminded to not concentrate on looking at the symptom but to look closer for the cause.
History & Subjective Complaints:
- 12 yr, Warmblood, Event horse, purchased to event at BE100 however has competed up to 1*
- So far that season had unfortunately posed some issues for my client, in particular the XC phase due to refusals.
- The rider had noticed that the saddle was not sitting straight but also that the mare’s hindquarters were not square.
- The saddle was therefore checked and the mare has received regular physio treatment from a registered Physiotherapist.
- Although there have been no other symptoms or lameness to cause any major concern my client wanted a fully body screening in order to check the whole body with the aim of finding an explanation to the poor performance.
SyncEquine Veterinary Report Highlighted:
Forelimbs:
- Bilateral hyperthermia of the palmer metacarpal is observed on medial (inside) and lateral views at rest and post exercise L>R
- Bilateral inflammation of the metacarpophalangeal joints pre and post exercise.


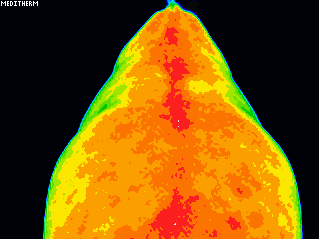
Body:
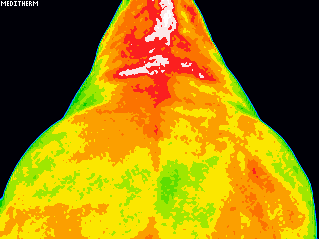
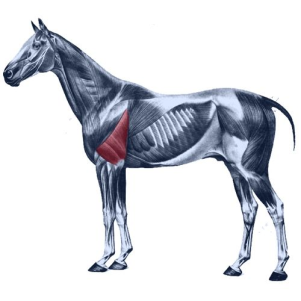
- There is a distinct bilateral focus of inflammation on lateral views of the upper body in the caudal aspect of the lateral shoulder region, apparent post exercise.
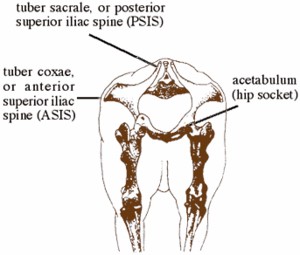
Hindlimbs:
- There is diffuse hyperthermic asymmetry of the left gluteal region on dorsal views of the hindquarters at rest
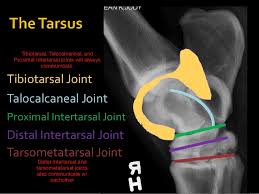
- Focal intertarsal inflammation is observed on dorsal (back)) and medial views of the hocks at rest and post exercise
- There is focal inflammation on the plantar aspect of the left tarsometatarsal joint
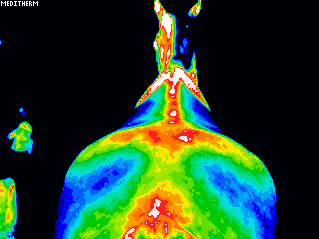
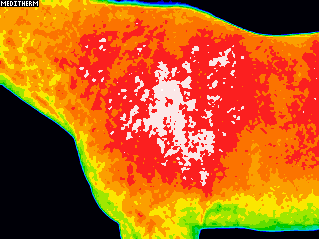
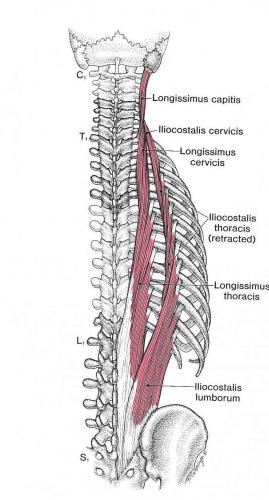
Spinal:
- There is focal inflammation of the cranial thoracic vertebrae and left thoracic trapezius musculature – this is more apparent post exercise.
Discussion
- Palmer metacarpal hyperthermia may not be significant in the absence of clinical signs of tendon or ligament pathology, these images may be used as a baseline for further monitoring
- If positive to flexion tests, further clinical correlation of front fetlock and tarsal joint inflammation is advised. Such thermal patterns can represent degenerative joint disease and this should be investigated if there is clinical concern
- Bilateral focal inflammation of the caudolateral shoulders is suspected to be secondary to saddle fitment and may explain saddle slippage
- Left gluteal hyperthermia at rest is suspected to represent muscular tightness through this region
- Cranial thoracic vertebral and left trapezius inflammation may also be linked to saddle figment. Spinal inflammatory patterns can, in some cases, be indicative of dorsal overriding of the spinous processes – however this would be unusual in the cranial thoracic region. This should however be investigated, if there is clinical concern.
Follow Up:
My client subsequently had her mare diagnosed further by her vet and the early onset of osteoarthritis was indeed suspected in the front fetlock joints. Which was then treated with corticosteroid injections. They together then went on to successfully finish the eventing season by going clear cross country.
During the winter the mare was also diagnosed with osteoarthritis in the both hocks and so my client decided to retire her from competing and concentrate on competing her other horses
Conclusion
There is no doubt in my mind that the cause of the poor performance was due to the mare experiencing pain in her front fetlocks. I am also certain that the tightness in the mare’s shoulders and left hind quarters was secondary to osteoarthritis in the fetlocks and hocks. The issue in the upper back may also have been linked but there was also the plausible explanation of the saddle fitting, which the owner had already addressed.
Case 2 June 2-17 – Pain or Behaviour
The reason the owner called for a consultation about her competition driving pony was to determine whether indeed the reason for the change in his behaviour when ridden was caused by pain.
History & Subjective Complaints:
- Predominantly a competition driving pony, also ridden under saddle
- Nov 16 – started bucking whilst ridden – physio identified a spasm in right hind quarter and left shoulder
- April 17 – referral to vet, declared sound so to carry on working and have regular physio treatment
- Barefoot but worked in hoof boots
Body:
- Focal inflammation of the *CT is observed on right lateral views of the neck pre and post exercise (*Cervical Thoracic Junction – Neck to Upper Back)
- No other significant thermal abnormalities observed.
Spinal:
- Focal inflammation of the caudal thoracic spine is observed on dorsal views of the back pre and post exercise


Feet:
- There is normal dorsal thermal symmetry of the forefeet and hind feet
- On palmer views, there is medial and lateral solar hyperthermic asymmetry of the left and right forefoot respectively
- Hyperthermic asymmetry of the right heel is observed on standing palmer views at rest, this is normal post exercise






Discussion:
- There is thermal evidence of mild foot imbalance in the forefeet – this improves after exercise. Thermal evidence suggests that there is a tendency to lean to the right and increase weight bearing on the right forefoot
- An assessment of the neck is advised – focal inflammation at the level of the CT junction may indicate muscular or spinal dysfunction at this level
- Inflammation of the caudal thoracic spinal region warrants further clinical correlation as this thermal pattern may represent muscular tightness through this region, spinal ligamentous sprain, or in more serious cases – dorsal overriding of the spinous processes (kissing spine)
Follow Up, 1 Week Post Scan
Feedback from Client following Owner’s Vet Assessment:
- Full workup performed and observed as sound on both hard and soft going
- However in canter in the arena, very tight, rigid back with no movement
- Evidence to justify x-raying the back
- X-ray showed there to be no areas of concern in the lumbar region with regular even spaces between each of the spinous processes
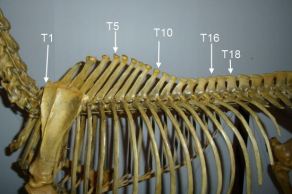
- The thoracic spine looked good with the exception of an impingement between T10 & T11.
- Vet did also note that there was a lot of tension in right side of Alfie’s neck (T1 area)
Follow Up 2 Days Later:
- Nerve blocked offending vertebrae (T10 & 11)
- The change in way of going was significant, much more free through the shoulder, worked with a much longer stride, and easily maintained left canter
- Still looked tight over the sacroiliac, but with the amount of tension and spasm he had there it’s not surprising
Follow Up 2 Weeks Later:
- Surgery performed (a wedge oseteotomy) being the best option
- Injecting with steroid may have given short term relief but wouldn’t resolve the problem long term
- Also had mild laminitis when given prednisolone to treat a respiratory infection a couple of years ago, so it would be too risky to medicate with steroids again.
- 3 -4 month rehab program, but hopefully this should make him a lot more comfortable and resolve the neck issue too
Four Months Later:
Significant improvement and successfully returning back to competing!
Conclusion
As owners we obviously know our equine partners very well as we work with them and see them on a regular basis. So if your horse’s behaviour changes of course it makes perfect sense to not ignore it but to investigate further. At the very least to rule out whether your horse is in pain.
In this case yes the pony was clearly in pain which due to the location of the impingement in the thoracic spine, was not surprisingly more noticeable when ridden and when the pony showed his discomfort by bucking. However as vets it is very difficult to make a diagnosis especially when there is no obvious lameness or discomfort. But as owners we also have to follow our gut when we know that our horse just isn’t comfortable. This is when our screening service proves an excellent tool to isolate areas of pain. Effective even more when used in conjunction with the vet’s diagnosis. Which in this case was literally a pain in the neck, no doubt connected to the upper back (T10 & T11) which in turn would explain the tightness over the sacroiliac.
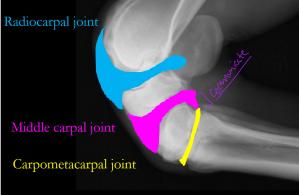
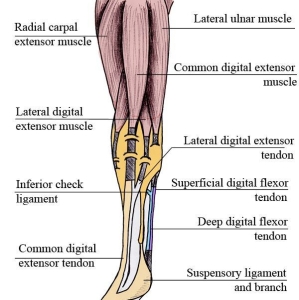
Case 3 October 2017 – Tendon & Ligament
Injuries are common in the key tendons which run like cables down the back of the lower leg (deep and superficial digital flexor tendons). These tendons extend from muscles high in the leg to the foot. When the muscles contract, they flex the leg. They also help support the leg and come under huge stress when a horse gallops, jumps or does any sort of athletic maneuver.
In the following case, the client’s vet suspected damage to the left fore suspensory ligament. However as the nerve block was inconclusive he endorsed using our screening service to see if we could pinpoint the area of concern.
History & Subjective Complaints:
- 10 yr old, TB, Ex Racehorse
- slipped in the field about 8-10 weeks ago, evidence of which could be seen by skid marks and a broken fence
- After which he did not feel or look quite right
- The vet attempted nerve blocking but could not block sound and no difference was seen
- However suspected damage to the origin of the suspensory ligament (where it attaches to the back of the knee)
- Vet recommended six weeks of box rest and three sessions of shock wave over two weeks
- During the walking exercise of the rehab programme, his owner noticed that he didn’t look sound
- Vet re blocked behind the knee which resulted in improving soundness but still not 100%
- Recommended now to have further diagnostics, X-Ray, Ultra Sound and MRI
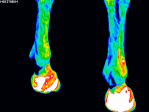
Forelimbs:
- Significant focal intercarpal inflammation is observed on dorsal views of the left carpus pre and post exercise. On lateral views there is diffuse hyperthermic asymmetry of the left carpus
- A small focus of inflammation is observed on lateral views of the *proximal left metacarpus
- On palmer carpal views, there is focal inflammation of the medial aspect of the radiocarpal joint
* Proximal – closest to








Discussion:
- There is no thermal evidence of pathology at the proximal attachment of the suspensory ligament
- The primary thermal finding is inflammation of the left dorsal intercarpal region with diffuse generalised hyperthermic asymmetry of the left carpus
- There is also focal inflammation of the left metacarpus, *distal to the carpometacarpal joint – Further imaging to determine the cause of inflammation is recommended
* Distal – farthest away
Follow Up:: October 2017
Examination – diagnostic Testing, Radiographs L Carpus & Ultrasonography:
Information for Owner
Our examinations have identified a multi-site lameness, partially referable to the carpus (knee) and the carpal sheath, where a lesion in the superficial digital flexor tendon has been identified.
Information for Referring Vet
The diagnostic imaging findings are in agreement with the results from diagnostic analgesia. (nerve block)
Whereas we think that part of the lameness originates from the (distended) LF middle carpal joint
The tear in the LF SDFT is likely to be contributing to the lameness more substantially.
Ultrasonography:
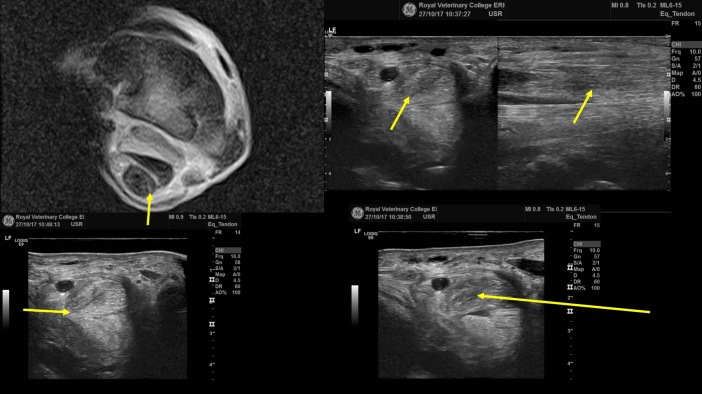
- The bone surface at the origin of the left fore suspensory ligament appeared irregular (enthesopathy), but the size and fibre pattern of the ligament was within normal limits. The lesion within the left fore SDFT at the level of the left fore superficial digital flexor tendon was identified as a distinct area of hypoechogenicity and altered fibre pattern distal to the musculotendinous junction and was associated with a partial transverse split of the tendon at this level – Diagnosis: Superficial digital flexor tendinitis
Conclusion:
This case resulted in complete correlation with the client’s vet and the subsequent referring equine clinic.
- The SyncEquine report highlighted inflammation of the left dorsal intercarpal region with diffuse generalised hyperthermic asymmetry of the left carpus.
- The equine clinic agreed that part of the lameness originated from the LF middle carpal joint.
- The SyncEquine report also identified a focal inflammation of the left metacarpus, *distal to the carpometacarpal joint.
- The ultra sound identified a lesion within the left fore SDFT at the level of the left fore superficial digital flexor tendon. (A distinct area of hypoechogenicity and altered fibre pattern distal to the musculotendinous junction was associated with a partial transverse split of the tendon at this level).
To find out how our screening service can detect ligament and tendon damage before reaching an acute level read more in next case
Case 4 Feb 16 & March 18 – Early Pathology
I was asked by Head Office if I could perform a follow up full body scan on this mare. The client’s veterinary practice were so impressed with our initial findings in February 2016 that they were keen to share this case with other veterinary practices. This was certainly another interesting case which further evidences the effectiveness of thermal imaging as an early diagnostic tool.
History & Subjective Complaints:
- Owner reported tendencies to ‘nap’ when turning on a tight circle to the left
- When jumping she also favoured the LF on landing.
- There were also some additional areas of concerns unrelated to the LF so a full body scan was completed.
Numerous areas of interest were reported on but the most significant finding was identified:
Forelimbs:
-
inflammation of the RF foot. Inflammation significantly increased post exercise on dorsal and palmer views


Discussion:
Assessment of the feet to rule out deep foot pathology was advised by our interpreting vet, alongside other observations.
Follow Up:
At the time of the first scan in February 2016, was sound so the findings in the RF were not considered significant by her vet. However in May 2016 the owner noted she was not comfortable weight bearing on the RF for extended periods of time, for example when putting studs in. In June 2016 Nimmy became lame in front, seemingly both front feet. Corns/bruising was suspected but it didn’t improve with treatment. Nimmy’s owner arranged for her front feet x-rayed in July 2016, these were clear so a period of rest followed. By mid August 2016 she appeared sound so gentle exercise commenced. After a successful start she became lame again in November 2016 following her first dressage competition. The treating vet completed nerve blocks which were inconclusive so in December 2016 an MRI of the forefeet was completed. MRI identified a 10 cm lesion of the RF deep digital flexor tendon (DDFT), the LF was normal.


Images show T1 HR transverse scan of the right fore foot showing a core lesion of the medial lobe of the deep digital flexor tendon.
March 2018 Report
History & Subjective complaints:
- The reason for the scan is as a follow up to a SyncEquine Full Body scan which was performed in February 2016, where subsequent veterinary report where deep foot pathology was identified in the Right Fore
- Further investigation via MRI in December 2016 detected a 10 cm lesion in the RF DDFT
- The owner requested a second SyncEquine scan to assess the current situation and then regular thermography scans to monitor progress and check coping with the rehabilitation plan
Forelimbs:
- Focal hyperthermic asymmetry of the palmer right metacarpophalangeal and pastern region is observed on lateral and palmer views at rest and post exercise.
Pre Exercise:
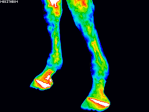


Post Exercise




Discussion:
- Significant hyperthermic asymmetry of the palmer right fore fetlock and pastern is likely to represent on-going tendonitis
- Thermal findings in the right forefoot are suggestive of on-going deep foot pathology (navicular?) but hyperthermia could be secondary to tendon inflammation
- Left forefoot solar hyperthermic asymmetry post exercise may be the result of lateral weight transfer from the right forelimb
Follow Up:
FURTHER INVESTIGATION: In January 2017 a RF Navicular Bursoscopy was performed revealing a synovial mass in the medial navicular bursa, associated with a long split of the medical lobe of the tendon and an erosion of the lateral lobe of the deep digital flexor tendon. The synovial mass was removed and the torn fibres debrided from the DDFT. Bone marrow was also collected for culture of stem cells which would be injected in the Navicular Bursa 1 month after surgery. Following a period of box rest, then in hand walking and restricted turnout, allowed unrestricted turnout in April 2017. Further stem cells and steroids were injected over July/August 2017, however a routine appointment found the horse still 1-2/10 lame in November 2017 so an MRI was booked for December 2017 which showed guarded improvement.
Conclusion:
Pathology was detected with physiological imaging during the early stages of investigation when the patient was presenting subtle changes. Isolating abnormality for further investigation was a success.
Summary
I hope you have found each of these cases as interesting as I have. For me the most satisfying aspect of my job is when my cases correlate with veterinary findings. What is even more rewarding is when my cases are added to the company’s case study portfolio. Which is constantly growing with more cases that evidence further the technology we use and the way we use it, certainly is proving it’s worth as a tool for the diagnostic tool kit. Along with being used for pain evaluation and treatment monitoring, of course benefits the equine veterinary industry by often resulting in being more cost effective to the owner, less stress for both the horse and owner and a much speedier diagnosis for all involved.
I will be sharing with you more cases in future blogs but in the meantime please make sure you like and follow our Facebook page (https://www.facebook.com/syncequine/) where you can see further cases which myself and other technicians are involved with.
If you are interested in finding out more about what our service offers or would like a free consultation please do not hesitate to contact us through our website: http://www.syncthermology.com



 Merehead and Emma Brinkworth, BCA BE90, June 18
Merehead and Emma Brinkworth, BCA BE90, June 18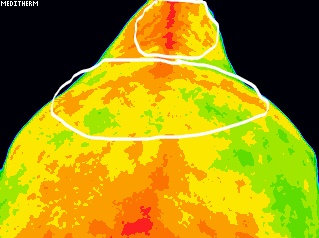




 September. I really was on the verge of giving up riding all together. However, my wonderful trainer who is also a great matchmaker introduced me to a little ex racehorse who was mine to have on loan to see how we get on. Well it has turned out that we get on very well. So much so that I am truly grateful to this little mare for returning my mojo.
September. I really was on the verge of giving up riding all together. However, my wonderful trainer who is also a great matchmaker introduced me to a little ex racehorse who was mine to have on loan to see how we get on. Well it has turned out that we get on very well. So much so that I am truly grateful to this little mare for returning my mojo. I always need a goal to keep me focused, whether achievable or not and a training plan to follow. So after swiftly changing my mind about giving up, I have kept busy schooling and training with Robyn, including the occasional show jump, dressage and arena eventing competition. So far nothing has fazed her and as she is also proving to be hugely talented with a massive heart. I decided to hell with it and register her BE this season.
I always need a goal to keep me focused, whether achievable or not and a training plan to follow. So after swiftly changing my mind about giving up, I have kept busy schooling and training with Robyn, including the occasional show jump, dressage and arena eventing competition. So far nothing has fazed her and as she is also proving to be hugely talented with a massive heart. I decided to hell with it and register her BE this season.